“Ever heard of a rhinovirus causing the common cold?”
A fun and approachable review of research: Bouzid, D., Hadad, O., Bertine, M., Houhou-Fidouh, N., Mirand, A., Duval, X., Bunel, V., Borie, R., Lucet, J. C., Descamps, D., & Visseaux, B. (2022). Rhinoviruses: Molecular diversity and clinical characteristics. International Journal of Infectious Diseases, 118, 144–149. https://doi.org/10.1016/j.ijid.2022.02.055
Written by
Vinaya Venkat

The Questions will be answered:
- What is a rhinovirus?
- Why is it important?
- Can it affect adults? If yes, how?
Psst – read this first!
COPD: Short form of Chronic Obstructive Pulmonary Disease
Co-infection: Infection with more than one pathogen at a time – any combination of bacterial, viral or fungal infection
Mono-infection: Infection by only one pathogen at a time
PCR: Short for Polymerase Chain Reaction – it is used to amplify the target genetic material to a level where it can be detected
A prequel of the research
‘Sniff, sniff, I have a runny nose again – thought 12-year-old me sitting on the bus to school. Thinking back to the times I had had a common cold this year alone, I wondered why I fell ill so often. During computer class, I was curious and read about the causes of the common cold. There I came across the name – rhinovirus (aka. human rhinovirus), where the word “rhino” means nose in Latin!
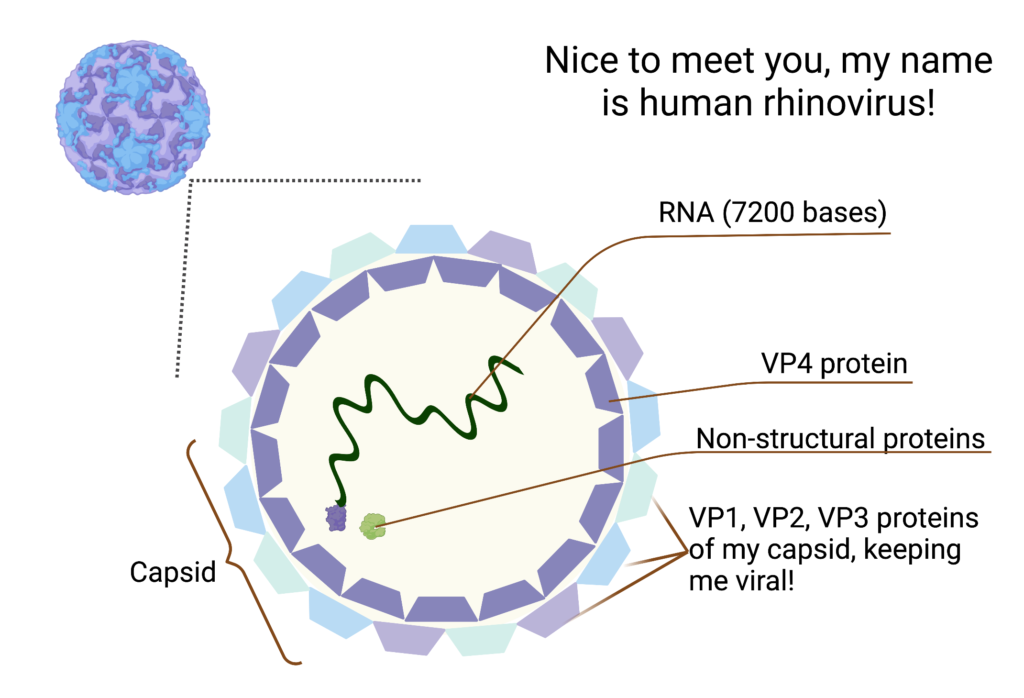
This virus was discovered by Dr Winston Price at John Hopkins University and collected from a sick hospital nurse! The first rhinovirus – formerly known as Johns Hopkins virus and now Human rhinovirus A1 – was swabbed from that nurse’s nasal passage. Being one of the smallest viruses (30 nm in diameter – which is 50 million times smaller than an ant!), it can pass through an FFP2/N95 mask. This might be why rhinovirus infections did not reduce as much as others like influenza during the pandemic despite social distancing measures.
The virus has a single strand of RNA as its genetic material, which is 7,200 bases long (bases, or nucleotides, are the units making up the genetic information) and stored in a capsid. The virus RNA produces only 11 proteins – of which VP1, VP2, VP3 and VP4 form the capsid structure. In contrast, the others help in virus replication and assembly in our body’s cells. Rhinovirus has over 100+ serotypes divided into three groups – Rhinovirus A, B and C.[1,2]
As I grew older, my passion for understanding how the common cold virus affects people increased. I took Sciences and studied virology. When looking for people who study rhinoviruses, I was stuck. Older researchers who studied the virus had retired from their labs and newer labs had shifted their focus to other emerging viruses perceived to have a greater public threat – especially to SARS-CoV-2 because of the COVID-19 pandemic.
Now at 22, still curious as ever about rhinoviruses, I came across literature about rhinovirus studies at daycares or as part of surveillance of respiratory diseases where the virus was studied as part of a cluster of respiratory viruses. Is no one curious about rhinoviruses anymore? They are so different in themselves. What about the various serotypes affecting healthy adults, and not just children?
Few are interested in this virus as it is relatively harmless. But recently more interest has been shown, after discovery of the link of rhinovirus C infection to increasing asthma severity, especially if contracted in childhood. Despite the mortality being almost zero and morbidity low, there is a massive global impact of the common cold leading to absences of employees from work [4].
Despite the common cold being so common, there is still no cure. There have also been attempts to design vaccines against the virus with no success due to the huge virus diversity (in serotypes) and the lack of a suitable study model [2]. Molecular techniques (designed to look for proteins or nucleic acids associated with the pathogen) have been designed to differentiate between rhinovirus groups. However, their clinical difference (disease-related signs) is still unclear. Epidemiological studies have mainly been conducted on children, making it difficult to generalise the effects on adults. [3]
This piece aims to characterise the diversity of rhinovirus infections in adults and if this diversity is reflected in the signs and symptoms displayed by the adults affected by these viruses. Now diving into the article and its work.
Nice plots and what do they really mean
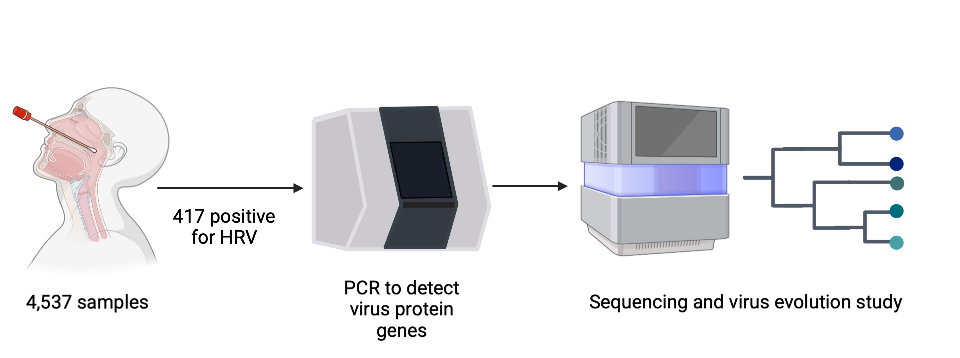
4,537 patients visiting hospitals in France, coughing and sneezing and complaining of the flu, were sampled and only 417 (9%) of these were positive for rhinovirus (Fig 1). These samples were checked for the virus’s protein-producing genes. They have then been sequenced to identify the exact rhinovirus isolate. A phylogenetic tree was designed to represent the diversity of the virus found in this population.
Alongside the PCR testing, clinical studies – which include observation of signs of illness displayed by the patient and their medical history – were also conducted on 178 patients (Fig 2). 56% suffered from chronic respiratory diseases such as asthma and COPD or were immunocompromised by lung transplantations. Meanwhile, 31% were neither immunocompromised nor had any chronic respiratory diseases.

112 out of 178 patients were admitted for respiratory distress or pneumonia (Fig. 2). 32 were admitted to the Intensive Care Unit (ICU), and eight died during their hospital stay. Any signs of co-infection were also marked as part of the clinical observation. A combination of co-infections was observed – 32 bacterial, 12 viral and 13 bacterioviral. Fungal co-infections were rarely observed. Patients infected with mono-infection were immunocompromised and had a chronic respiratory disease.
To understand how the virus was dispersed in the study population, researchers sequenced the samples collected from these patients. Out of 186 sequences, 98 belonged to HRV-A, 27 belonged to HRV-B and 61 to HRV-C (Fig 3).
The researchers not only studied virus diversity in the population but also could differentiate between rhinovirus A, B and C infections through patient symptoms. Among all the viruses, HRV-A infections were more common in the study populace and associated with increased pneumonia. HRV-B cases were frequently observed in immunocompromised patients, leading to ICU admissions. HRV-C cases were mainly associated with asthma exacerbations and less with pneumonia.

With the description of these infection patterns and their study to characterise them to their respective virus groups, this information would help assess the burden of HRV infections in adults. One limitation of the study is that the target was hospitalised patients (admitted due to severe/chronic respiratory disease) who were vulnerable to hospital-acquired infections. So the study results cannot be generalised for healthy adults.
In a healthy adult population, a rhinovirus infection would clear out within hours or a couple of days. This makes it difficult to detect the virus in sufficient quantities to sequence and identify. Prior exposure to other serotypes causes bias in adult populations to present with viruses not normally circulating in the region. Keeping the following hurdles in mind, studies are needed to understand the infection patterns in a generally fit adult population.
Take-home messages
- Rhinoviruses are the leading cause of common colds – especially in children. Hence, not much is known about common colds in adults.
- Though generally harmless, rhinoviruses have been linked to aggravation of respiratory ailments such as pneumonia, asthma and COPD.
- Out of the classified groups, rhinovirus A is found frequently in the population, followed by rhinovirus B and then rhinovirus C.
- HRV-A has been associated with increased pneumonia, HRV-B in immunocompromised individuals, and HRV-C with asthma exacerbation.
More studies are required on how rhinovirus affects a healthy adult population due to the economic impact of its infections.
Links
Original thesis/article:
Bouzid, D., Hadad, O., Bertine, M., Houhou-Fidouh, N., Mirand, A., Duval, X., Bunel, V., Borie, R., Lucet, J. C., Descamps, D., & Visseaux, B. (2022). Rhinoviruses: Molecular diversity and clinical characteristics. International Journal of Infectious Diseases, 118, 144–149. https://doi.org/10.1016/j.ijid.2022.02.055
References:
- Jacobs, S. E., Lamson, D. M., St. George, K., & Walsh, T. J. (2013). Human Rhinoviruses. Clinical Microbiology Reviews, 26(1), 135–162. https://doi.org/10.1128/cmr.00077-12
- Kennedy, J. L., Turner, R. B., Braciale, T., Heymann, P. W., & Borish, L. (2012). Pathogenesis of rhinovirus infection. Current Opinion in Virology, 2(3), 287–293. https://doi.org/10.1016/j.coviro.2012.03.008
- Varela, F. H., Sartor, I. T. S., Polese-Bonatto, M., Azevedo, T. R., Kern, L. B., Fazolo, T., de David, C. N., Zavaglia, G. O., Fernandes, I. R., Krauser, J. R. M., Stein, R. T., & Scotta, M. C. (2022, April). Rhinovirus as the main co-circulating virus during the COVID-19 pandemic in children. Jornal De Pediatria. https://doi.org/10.1016/j.jped.2022.03.003
- Bramley TJ, Lerner D, Sames M. Productivity losses related to the common cold. J Occup Environ Med. 2002 Sep;44(9):822-9. doi: 10.1097/00043764-200209000-00004. PMID: 12227674.
Could be interesting to read:
This book gives a concise review of all the information about the developments in the field of rhinoviruses – https://www.sciencedirect.com/book/9780128164174/rhinovirus-infections#book-description
A must-see pokemon card but for HRV 16! https://web.stanford.edu/group/virus/retro/2000/humanrhinovirus16.html